TIC
Description
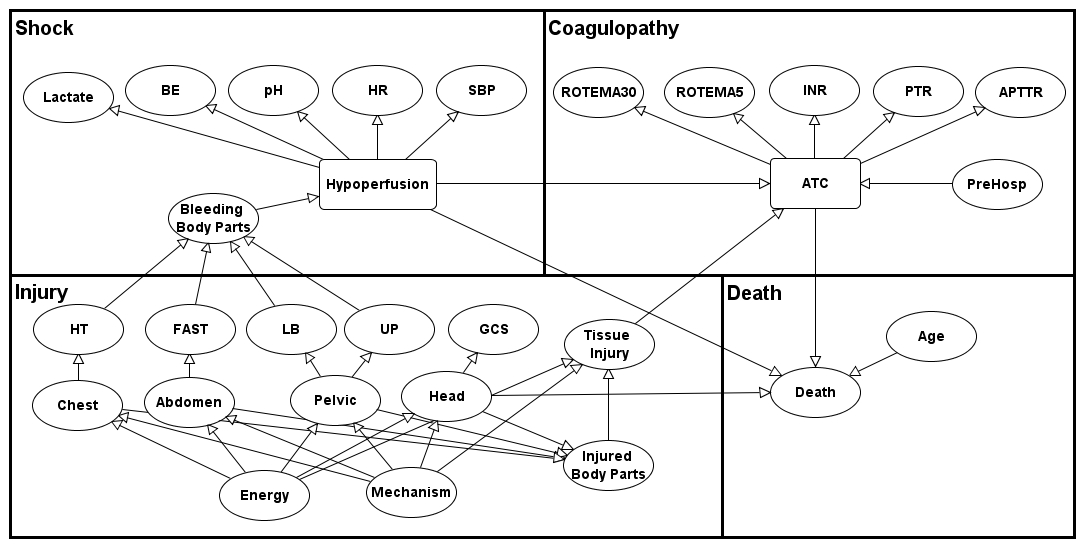
Trauma Induced Coagulopathy (TIC) is an endogenous impairment of clotting ability that occurs after a combination of tissue hypooperfusion and tissue injury.
Evidence
The method for classifying the TIC states is described by Yet et al (2013).
Excluded BN Elements
Hypothermia is independently associated with coagulopathy (Cohen et al., 2013; Cosgriff et al., 1997; Mitra et al. 2011; Wafaisade et al. 2010). Moderate and severe hypothermia (less than 33) impairs fibrin synthesis, thrombin generation and platelet function with significant effects on function and clinical bleeding observed (Wolberg et al., 2004; Martini et al., 2009; Meng et al., 2003). Pig models Martini et al., (2005) and Martini, 2007) found significant relation with coagulopathy and severe hypothermia (32C).
Brohi et al. (2008) observed no significant difference in laboratory clotting tests or thrombin generation betweeen normothermic and mildly hypothermic (34 - 35 C) trauma patients. Therefore, trauma induced coagulopathy is not due to mild hypothermia according to Brohi et al. (2008). A variable about hypothermia is not included in our model since our development and validation cohort is mainly consists of normothemric and mildly hypothermic patients (>34). Only 2% of the patients were moderately hypothermic (34-32 C) and there were no severely hypothermic patients. In our cross and external valdation, the BN could accurately predict TIC for hypothermic patients using other markers of hypoperfusion.
Acidemia is found to be associated with coagulopathy in several studies (Cohen et al. (2013), Cosgrif et al. (1997) and Niles et al. (2008)). Several animal models (swine) also reported that acidemia causes coagulopathy and accelerates fibrinogen consumption (Martini et al., 2005; 2007). In Human in-vitro studies, Engstrom et al. (2006) observed strong correlation between pH levels and coagulopathy, and Meng et al. (2003) observed reduced Factor VIIa activity at pH 7.0.
However, it is very difficult to separate the effects of acidemia from those of shock and hypoperfusion. The possible effects of acidemia on coagulation function appears not to be reversible by simple correction of the acidosis. According to Brohi et al. (2007a; 2008) trauma induced coagulopathy is not due to coagulation dysfunction because of acidosis; the main driver of coagulopathy appears to be hypoperfusion. Therefore we did not modelled variables related to acidemia (such as pH) as a direct cause of coagulopathy. These variables are correlated with coagulopathy through hypoperfusion variable in our model.